HOME
ABOUT
▲
MEET THE STAFF
SFA BOARD OF DIRECTORS
FOUNDERS VIDEO
STRATEGIC PLAN
2024 ANNUAL REPORT
▲
2023 ANNUAL REPORT
2022 ANNUAL REPORT
2021 ANNUAL REPORT
2020 ANNUAL REPORT
2019 ANNUAL REPORT
CRISIS
SERVICES
▲
ASSESSMENT
OUTPATIENT SERVICES
CHILDREN AND FAMILY SERVICES
WOMEN’S RESIDENTIAL TREATMENT
MEN’S RESIDENTIAL TREATMENT
RECOVERY RESIDENCE
ADMISSIONS
SLIDING FEE SCALE APPLICATION
UPLOAD DOCUMENTS
NOTICE OF PRIVACY PRACTICES
EVENTS
▲
RENTALS
WAYS TO GIVE
▲
GENERAL GIVING
FREEDOM FIGHTERS – MONTHLY GIVING
TREATMENT BOOK SPONSOR
FREQUENCY OF HOPE IMPACT CAMPAIGN
CLIENT CHRISTMAS
LEGACY & PLANNED GIVING
TESTIMONIES
▲
FIND US ON YOUTUBE
EMPLOYMENT
SWAG STORE
CONTACT US
▲
MAT-SU OFFICE 907-373-4732
HOMER OFFICE 907-416-7569
CLIENT PAYMENTS
▲
HOUSING PAYMENTS
TREATMENT SERVICE PAYMENTS
GIVE
Get Our Newsletter!
Set Free Alaska
Mat-Su Office 907-373-4732
Homer Office 907-416--7569
GIVE
Get Our Newsletter!
HOME
ABOUT
MEET THE STAFF
SFA BOARD OF DIRECTORS
FOUNDERS VIDEO
STRATEGIC PLAN
2024 ANNUAL REPORT
2023 ANNUAL REPORT
2022 ANNUAL REPORT
2021 ANNUAL REPORT
2020 ANNUAL REPORT
2019 ANNUAL REPORT
CRISIS
SERVICES
ASSESSMENT
OUTPATIENT SERVICES
CHILDREN AND FAMILY SERVICES
WOMEN’S RESIDENTIAL TREATMENT
MEN’S RESIDENTIAL TREATMENT
RECOVERY RESIDENCE
ADMISSIONS
SLIDING FEE SCALE APPLICATION
UPLOAD DOCUMENTS
NOTICE OF PRIVACY PRACTICES
EVENTS
RENTALS
WAYS TO GIVE
GENERAL GIVING
FREEDOM FIGHTERS – MONTHLY GIVING
TREATMENT BOOK SPONSOR
FREQUENCY OF HOPE IMPACT CAMPAIGN
CLIENT CHRISTMAS
LEGACY & PLANNED GIVING
TESTIMONIES
FIND US ON YOUTUBE
EMPLOYMENT
SWAG STORE
CONTACT US
MAT-SU OFFICE 907-373-4732
HOMER OFFICE 907-416-7569
CLIENT PAYMENTS
HOUSING PAYMENTS
TREATMENT SERVICE PAYMENTS
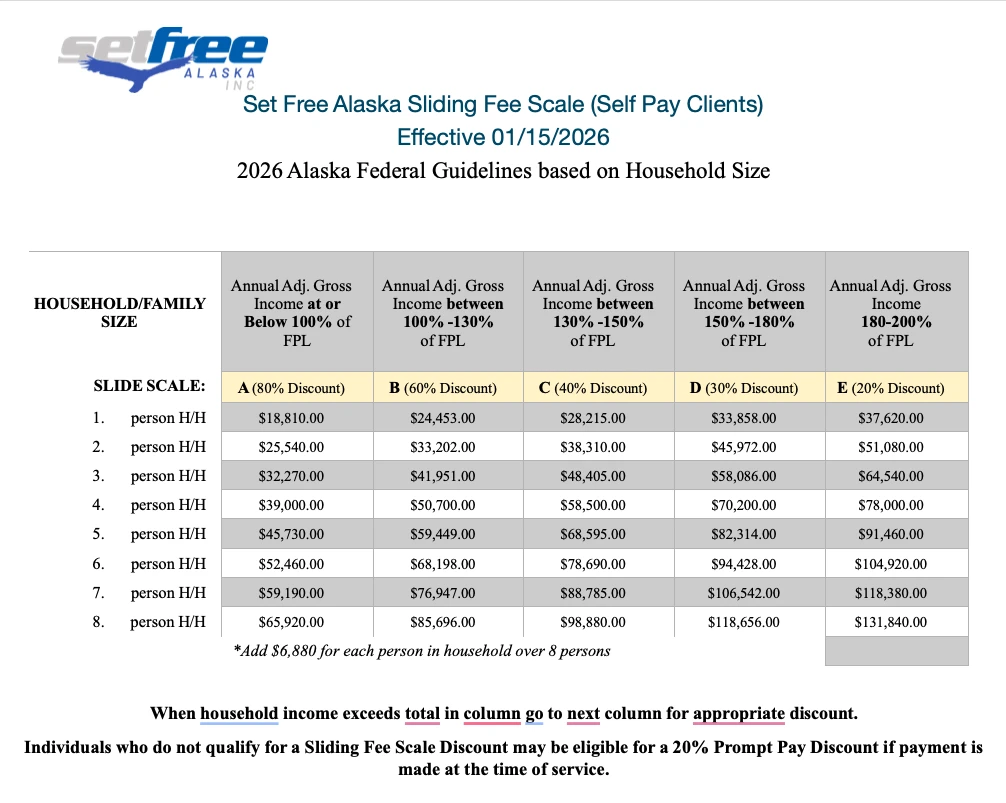
SLIDING SCALE FEE APPLICATION
This application is used to determine eligibility for the Sliding Fee Scale Program, which provides discounted rates for services based on household income and size, for individuals without insurance, or those with underinsured plans. Please complete the form and provide the required documentation to apply.
Application Date
(Required)
MM slash DD slash YYYY
Client Name
(Required)
First
Last
Date Of Birth
(Required)
MM slash DD slash YYYY
Email
(Required)
Address
(Required)
Street Address
City
State / Province / Region
ZIP / Postal Code
Source Of Income ( Select All That Apply )
(Required)
SSI
SSDI
Unemployment
Public Assistance
Place Of Employment
No Income ( Must complete “No Income Attestation” form )
Other
Please Explain Other From Above
Medicaid Application Date:
Approval Date:
Medicaid Application Method:
Online
Paper
DPA Office
Medicaid Denial Date:
Medicaid Denial Reason:
Attach Proof Of Income
Proof of gross household income is required for all family members to include proof of items that apply including paystubs, benefit award letters, and self-employment ledgers or returns. Sources of income, include but not limited to, wages, salaries, tips, taxable amount of pension, annuity or IRA distributions, Social Security benefits, VA benefits, unemployment, state or federal assistance, child support, alimony, worker’s compensation benefits, rental income. For self-employed, provide a copy of the previous year’s income tax return, including the Schedule C.
Upload Files Here
Max. file size: 50 MB.
Family/Household Member Information (List Applicant Income First, Then spouse, and biological or legally adopted children under 18 years old.)
(Required)
First Name
Last Name
Date Of Birth ( MM/DD/YYYY )
Relationship To Self
Employer
Total Income Last 12 Months
Add
Remove
Press the + for additional rows.
Consent
(Required)
By clicking and signing below
• I acknowledge that the above and attached information is an accurate reflection of my household income. I understand that I am responsible for updating Set Free Alaska (SFA) of changes in income within 30 days. In addition, I understand that I am responsible for payment of services rendered at SFA, with or without a discounted rate.
• I permit the request for proof of income as noted above. I understand that more information may be required. All information provided will remain confidential under HIPAA federal regulations. Any discounts apply to all charges within the approved period for behavioral health and/or medical services provided by SFA.
If I qualify for Financial Assistance/discount:
• I understand that if I have not fully and correctly presented my household income or provided any false information, or if I have not disclosed my insurance coverage, I may lose or have a reduced discount rate. If I lose the discount, I agree to pay the balance on my account. I also agree to pay any legal fees for the collection process.
• I agree to repay any money if I receive other payment for the medical services covered. Such payments may include insurance payments, governmental program payments, and awards from a lawsuit.
• I agree to tell Set Free Alaska of any changes that could affect my eligibility, including changes to family size, income, and health insurance coverage. If I qualify for a public assistance program, I will apply to that program and provide Set Free Alaska with proof of application.
I agree to the above information.
Applicant Name
(Required)
First
Last
By entering your name, you are verifying that you are the applicant, and that all information entered is accurate to the best of your knowledge.
Date
(Required)
MM slash DD slash YYYY
Applicant Name If Not The Client
First
Last
By entering your name, you are verifying that your are submitting this application on behalf of the Applicant and with their knowledge. You also verify that the information entered is accurate to the best of your knowledge.
Phone
Sign Up For Our Newsletter!
Choose email list to be added to
Subscribe
First Name
Last Name
Email address:
Leave this field empty if you're human: